Minimally invasive interventions:
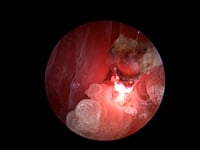
A variety of instruments can be passed through the rhinoscope, allowing the veterinary endoscopist to treat a range of abnormalities with little or no discomfort to the patient. The endoscopist can remove nasal foreign bodies (grass seeds, sticks), grass blades that have been vomited up over the soft palate in cats, fungal plaques (aspergillosis) and polyps, debulk tumours using special instruments placed through the operating port of the endoscope (e.g. lasers), debride dead turbinate tissue in cats with herpesvirus-induced rhinitis, stretch narrow areas at the back of the nose (nasopharyngeal stenosis) induced by chronic inflammatory conditions using a balloon catheter and/or laser, and use the fluid port on the endoscope for nasal/sinus flushing when continuous saline irrigation or antifungal treatment for aspergillosis is required.
Nasal Aspergillosis Treatment in cats and dogs involves endoscopic debridement combined with targeted antifungal soaks, eliminating the necessity for traditional sinus trephination. This method allows for direct visual access via transnasal routes, ensuring precise debridement and local antifungal application. The result is improved patient comfort, reduced recovery time, and enhanced treatment efficacy compared to conventional open surgical methods.